Total cholesterol
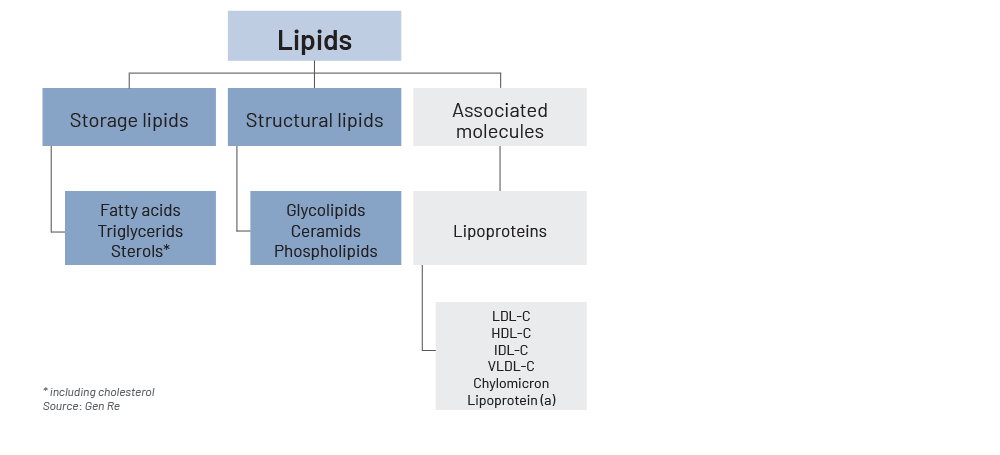
Total cholesterol includes LDL cholesterol, HDL cholesterol and cholesterol associated with triglyceride-rich lipoproteins. These include VLDL cholesterol, IDL cholesterol or remnant cholesterol. The measurement of TC is necessary to calculate the non-high-density lipoprotein (non‑HDL) cholesterol value (TC minus HDL=Non‑HDL).3
LDL cholesterol
Low-density lipoprotein consists of a molecule of apolipoprotein B (ApoB), other apolipoproteins, and a variable number of cholesterol molecules. There are different subtypes of LDL that differ in their atherogenic attitude, but a determination of LDL subtypes is not recommended, as the evidence regarding risk reduction through lipid lowering is based on the measurement of LDL cholesterol (and not its subtypes). Lowering the LDL cholesterol concentration is the primary treatment goal.4
HDL cholesterol
Similar to LDL cholesterol, different HDL subfractions can be distinguished, which differ in their apolipoprotein composition and also the amount of cholesterol transported. Low HDL cholesterol levels indicate inflammation or metabolic problems, especially diabetes and correlate with an increased risk of cardiovascular events.5
Triglycerides
Triglycerides are also transported on different lipoproteins, mostly on VLDL, chylomicrons and chylomicron remnants. The TG concentration correlates with the cardiovascular event rate, but the increased cardiovascular risk is not caused by triglycerides directly. Atherosclerotic pathogens are primarily the cholesterol contained in the TG‑rich lipoproteins such as VLDL, the particles themselves and the change of LDL and HDL metabolism, which is caused by the increased concentration of triglyceride-rich lipoproteins.
The risk associated with triglyceride-rich lipoproteins can be assessed by their amount of cholesterol (e.g. VLDL cholesterol or remnant cholesterol) or the ApoB level. The cholesterol associated with TG‑rich lipoprotein cholesterol is included in the non‑HDL cholesterol parameter.6
Non‑HDL cholesterol
Non‑HDL cholesterol is a calculated parameter: TC minus HDL. Non‑HDL summarises all cholesterol that cannot be assigned to HDL, i.e. is transported in ApoB-containing lipoproteins. This includes the cholesterol contained in the TG‑rich lipoproteins such as VLDL in addition to LDL and Lp(a). It is assumed that all ApoB-containing lipoproteins have a pro-atherogenic effect.
Non‑HDL cholesterol is therefore considered a global parameter for lipid-associated risk, similar to the ApoB concentration. The higher the serum TG values, the greater the superiority of non‑HDL cholesterol over LDL cholesterol in terms of risk stratification and therapy control. It is therefore particularly helpful to analyse non‑HDL cholesterol in patients with elevated TG levels.7
Lipoprotein (a)
Lipoprotein (a) levels are essentially genetically determined. The Lp(a) concentration is not normally distributed in the general population but is strongly shifted to the left (in the Gaussian distribution). This means that there are many people with very low Lp(a) levels and a few with excessively high levels. There are ethnic and gender-specific differences in Lp(a) concentration. Women have on average 5 to 10% higher Lp(a) values than men. Furthermore, renal dysfunction may increase Lp(a) values, while impaired liver function may lead to decreased Lp(a) plasma concentration. But most importantly, diet and physical activity have no influence and oral lipid-lowering drugs hardly affect Lp(a) levels.8
Apolipoprotein B
The plasma concentration of ApoB shows a close correlation with cardiovascular risk, similar to the non‑HDL cholesterol concentration. Determination of the ApoB concentration can be helpful to further clarify an “apparent” increase in LDL concentration in cholestatic liver diseases. If ApoB is also elevated in this situation, this indicates an actual increase in atherogenic lipoproteins. If the ApoB concentration is discordant with the LDL cholesterol concentration, this indicates the presence of abnormal lipoproteins, which is typical of cholestasis.9
Which lipids are of concern?
Different perspectives, different preferred lipid parameters
To decide which lipid parameter is “the best”, one must define the outcome of interest as this depends on what is being attempted by evaluating a lipid profile.
The primary focus in clinical practice is on defining the “right” moment for treatment, on determination of the most suitable type of treatment, and on monitoring hyperlipidaemia with the aim of reducing cardiovascular risks. In an insurance underwriting context, predicting all-cause and cardiovascular-specific mortality and morbidity risk is primarily relevant. Different lipid parameters have been shown to be better suitable for the two different objectives of (a) managing and monitoring treatment success, and (b) predicting absolute or relative cardiovascular risk.10,11
Treatment selection and monitoring perspective
Treatment success is defined as the effectiveness of a particular intervention in achieving a specific outcome. For example, a cholesterol-lowering medication in the clinical context is considered successful if it reduces LDL cholesterol levels to a certain target range.
Like other lipid parameters, LDL is associated with increased risk of atherosclerotic cardiovascular disease (ASCVD).12 People with primary elevations of LDL cholesterol are at a higher risk of ASCVD as a result of a long-term exposure to markedly elevated LDL levels, even in the absence of pre-existing ASCVD.13
LDL and/or non‑HDL are usually chosen as the preferred marker to monitor treatment success, as they are more responsive to treatment than other lipid parameters. For example, LDL and non‑HDL ranked highest for treatment response to initial statin treatment in a population with previous acute coronary syndrome.14
Lowering of LDL cholesterol is widely accepted as a key objective in the prevention of cardiovascular disease.15 As an example, the West of Scotland Coronary Prevention Study, a large randomised controlled trail with a 20‑year follow‑up of almost 7,000 men with high LDL levels identified a continued benefit from five years of lowering LDL cholesterol with a statin. It showed decreased mortality from cardiovascular causes and an ongoing reduction in cardiovascular hospital admissions.16
This positive effect has been confirmed by other studies. The proportional reduction in ASCVD achieved by lowering elevated LDL cholesterol depends on the absolute reduction in LDL cholesterol, with each 1 mmol/L reduction corresponding to a reduction of about 20% in ASCVD.17
Controversy remains about which people to treat and which goals to achieve, and about the extent of benefits and potential harms in the context of primary prevention.18
US population studies suggest that optimal total cholesterol levels are about 150 mg/dL (3.8 mmol/L), which corresponds to an LDL cholesterol level of about 100 mg/dL (2.6 mmol/L). Adult populations with cholesterol concentrations in this range manifest low rates of ASCVD.19 The European guidelines consider LDL cholesterol target levels of <116 mg/dl (3.0 mmol/L) as the target value.20
However, there is no “one” specific LDL cut‑off value that should not be exceeded. The amount of blood cholesterol allowed to circulate in the blood depends on age, sex and numerous other risk factors for cardiovascular diseases. These risk factors include obesity, lack of exercise, smoking, family history of lipometabolic disorders, family history of stroke or heart attack and high-fat diet.
Previous illnesses are also taken into account. Defined pre-existing conditions for which elevated LDL levels should be lowered include type II diabetes, high blood pressure, pre-existing vascular diseases (e.g. stroke, heart attack, etc.), elevated TG, liver steatosis or history of acute pancreatitis.21
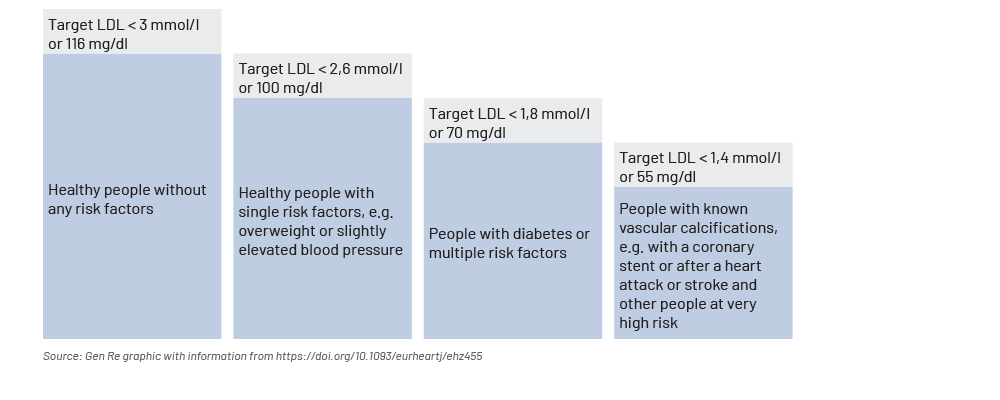
All major current guidelines on the prevention of ASCVD recommend an assessment of a total coronary vascular disease risk. Accordingly, different health risk groups result in different target values for LDL. As a general rule of thumb: the higher the number of a single risk for developing cardiovascular disease or with already existing cardiovascular diseases, the more intense the action should be to lower the target value for LDL levels (see Figure 2).
- For healthy people without any risk factors, an LDL cholesterol value <116 mg/dL (<3.0 mmol/l) is considered the target value.
- For healthy people with single risk factors, e.g. overweight or with slightly elevated blood pressure, the LDL cholesterol value should be <100 mg/dL (<2.6 mmol/l).
- Patients with diabetes or multiple risk factors should aim for an LDL cholesterol of <70 mg/dL (<1.8 mmol/l).
- For people with known vascular calcifications, e.g. with a stent in the coronary arteries or patients after a heart attack or stroke and other people at very high risk, the LDL cholesterol target value is <55 mg/dL (<1.4 mmol/l).22
Figure 2 – Guideline values in the management of cholesterol levels